

TRT is often framed around the idea of achieving “stable” testosterone levels, with frequent injections promoted as a way to reduce fluctuations. However, this concept does not reflect how injectable testosterone behaves in the body.
Rather than producing steady concentrations, testosterone esters follow predictable patterns of rise and decline. This article explains why true stability is biologically unattainable and why the appearance of “stable levels” is largely an illusion.
The Concept of “Stable Levels” and Its Clinical Appeal
The idea of maintaining “stable” testosterone levels in TRT is widely accepted in both clinical practice and patient communities. Increasing injection frequency — from weekly to more frequent protocols — is commonly believed to produce a more consistent hormonal environment and reduce fluctuations in mood, libido, and energy.
This idea makes intuitive sense, but it doesn’t accurately reflect how physiology works. Natural testosterone levels are not truly stable — they fluctuate throughout the day and are released in pulses driven by luteinizing hormone, resulting in constant variation rather than a flat, steady level.
In TRT, the idea becomes even less accurate. Injectable testosterone doesn’t stay at a steady level — it rises after an injection, reaches a peak, and then gradually declines as the body processes it.
Because of this, “stable levels” isn’t a true physiological state, but a simplified way of describing smaller fluctuations. In reality, the levels are still constantly changing — just within a narrower range.
Why Flat Levels of Testosterone Are Biologically Impossible
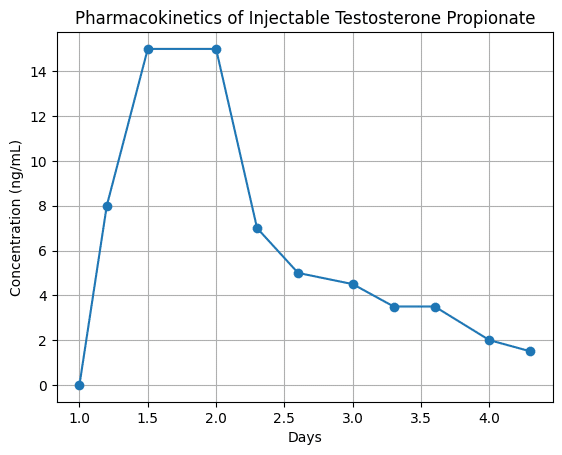
All injectable testosterone esters follow the same basic pharmacokinetic rule: exponential elimination. After an injection, testosterone levels rise as the compound is absorbed and converted, reach a peak (Cmax), and then steadily decline as the body clears it. This process is not linear and never produces a true plateau.
The concept of half-life is often misunderstood here. Half-life does not mean stability — it simply describes how long it takes for the concentration to drop by 50%. It does not imply that levels:
- remain constant;
- reach a plateau;
- or “even out” over time.
At no point do levels actually level off. Instead, they are always changing, following a continuous downward curve.
As a result, every injection creates the same pattern: a peak followed by a gradual decline. The speed of this decline depends on the ester (e.g., enanthate vs cypionate), but the overall behavior is the same. Longer esters only slow the process — they do not make levels stable.
The key implication is straightforward: a flat, stable testosterone level is not achievable with injectable formulations. The body is constantly metabolizing and clearing the hormone. What appears as “stability” is actually a series of overlapping decline curves, not a steady state.
| Ester | Approximate Half-Life | Time to Peak (Cmax) | Elimination Pattern |
| Testosterone Propionate | ~2 days | 24–48 hours | Rapid peak → rapid decline |
| Testosterone Enanthate | ~4–5 days | 48–72 hours | Moderate peak → gradual decay |
| Testosterone Cypionate | ~5–6 days | 48–72 hours | Moderate peak → gradual decay |
| Testosterone Undecanoate (IM) | ~20+ days | ~5–7 days | Delayed peak → prolonged decay |
Dose Overlap and the Illusion of Stability
When testosterone is administered repeatedly, each new dose is introduced before the previous one has been fully eliminated. This results in dose overlap, a pharmacokinetic phenomenon known as superposition. Rather than producing a flat concentration, repeated dosing creates a series of overlapping curves, where residual levels from prior injections combine with newly administered hormone.
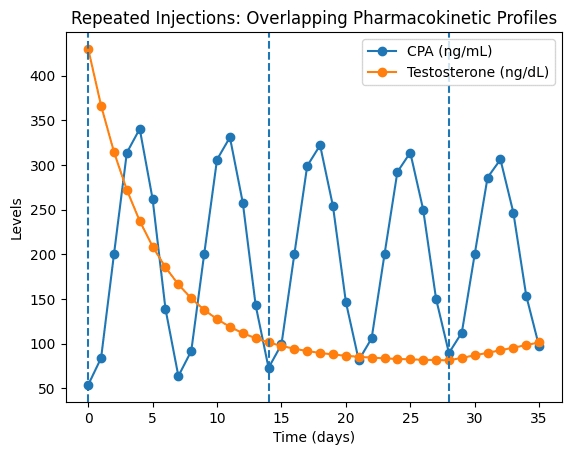
Increasing injection frequency changes the shape of these curves, but not their fundamental nature. As dosing becomes more frequent, individual peaks become smaller and troughs less pronounced. However, fluctuations do not disappear — they are merely compressed into narrower ranges. The underlying pattern remains a continuous sequence of peaks and declines governed by exponential elimination (PubMed; FDA).
This creates the illusion of stability. On standard lab testing or subjective perception, hormone levels may appear “steady,” particularly when measured between peak and trough extremes. In reality, the system is still dynamic, with concentrations constantly rising and falling — just within a reduced amplitude.
Effect of Injection Frequency on Peak–Trough Variation
While higher-frequency protocols reduce visible variability, they do not eliminate it. Instead, they transform large fluctuations into smaller, more frequent oscillations. From a pharmacokinetic perspective, this is not true stability, but a smoothing of the curve through cumulative overlap.
| Injection Frequency | Peak Amplitude | Trough Depth | Apparent Stability | Actual Pharmacokinetic Behavior |
| Weekly | High | Low | Low | Large peak–trough fluctuations |
| Twice weekly | Moderate | Moderate | Moderate | Reduced but persistent variation |
| Every other day | Lower | Higher | High | Compressed fluctuations |
| Daily | Minimal | Elevated | Very high | Continuous micro-fluctuations |
This distinction is critical. What is often interpreted as “stable levels” is, in reality, a visual or statistical artifact of reduced peak–trough amplitude — not the absence of fluctuation. The system remains in constant motion, with each dose contributing to an ongoing cycle of absorption and elimination.
In this sense, stability in TRT is not a physiological state, but an optical illusion created by overlapping decay curves.
Why Protocols Behave Differently Across Patients
Testosterone pharmacokinetics are not uniform across individuals. Even when identical compounds and dosing schedules are used, serum levels and clinical responses can vary significantly due to differences in binding proteins, metabolism, and receptor sensitivity.
Key sources of variability include:
- Sex hormone-binding globulin (SHBG) — regulates the fraction of free, biologically active testosterone
- Hepatic metabolism — determines how quickly testosterone esters are processed and cleared
- Enzymatic activity — affects conversion pathways and elimination rates
- Androgen receptor sensitivity — influences how strongly tissues respond to the same hormone level
SHBG plays a central role in modulating free testosterone availability. Individuals with higher SHBG may exhibit lower free fractions despite similar total levels, while those with low SHBG may experience greater fluctuations in bioavailable hormone. In parallel, hepatic metabolism and enzymatic activity influence how quickly testosterone esters are cleared, altering both peak intensity and rate of decline (National Institutes of Health; PubMed).
At the tissue level, variability in androgen receptor sensitivity further decouples serum concentration from biological effect. As a result, two patients on the same protocol may present with markedly different hormonal profiles and subjective outcomes.
This variability challenges the notion of a universally “optimal” or “stable” protocol. What appears stable in one individual may produce noticeable fluctuations or suboptimal effects in another.
The Risks of Chasing “Stable Levels” in TRT Optimization
The pursuit of perfectly “stable” testosterone levels has led to increasingly aggressive dosing strategies, often involving very frequent injections in an attempt to eliminate fluctuations. While this may reduce visible peak–trough variation, it does not remove the underlying pharmacokinetic dynamics — and can introduce new problems.
One of the primary risks is unnecessary protocol complexity. Increasing injection frequency adds logistical burden, reduces adherence, and creates more variables without fundamentally changing how testosterone behaves in the body. Absorption and exponential elimination remain unchanged, meaning the system is still inherently dynamic.
There is also a tendency to over-optimize laboratory numbers at the expense of clinical outcomes. A visually smoother concentration curve may appear “better” on paper, but does not guarantee improved symptom control, well-being, or hormonal balance. In some cases, excessive focus on stability can distract from more relevant factors:
- estradiol regulation;
- hematological parameters (e.g., hematocrit);
- lipid profile changes;
- individual sensitivity to androgens.
Finally, the attempt to eliminate all fluctuations reflects a misunderstanding of physiology. Hormonal systems are not static, and forcing an artificial sense of “stability” does not inherently improve biological outcomes.
Conclusion
Stable testosterone levels are not achievable with injectable TRT. All protocols produce continuous fluctuations driven by absorption and exponential elimination.
More frequent dosing may smooth the curve, but it does not eliminate variability — only reduces its amplitude. What appears as stability is simply a compressed pattern of ongoing change.
Stability in TRT is not a physiological state, but a simplified interpretation of inherently dynamic hormone levels.